Category: 80by2018blog

NEW!
Interview with ScreeND – 2026 National Achievement Award Grand Prize Winner
NEW!
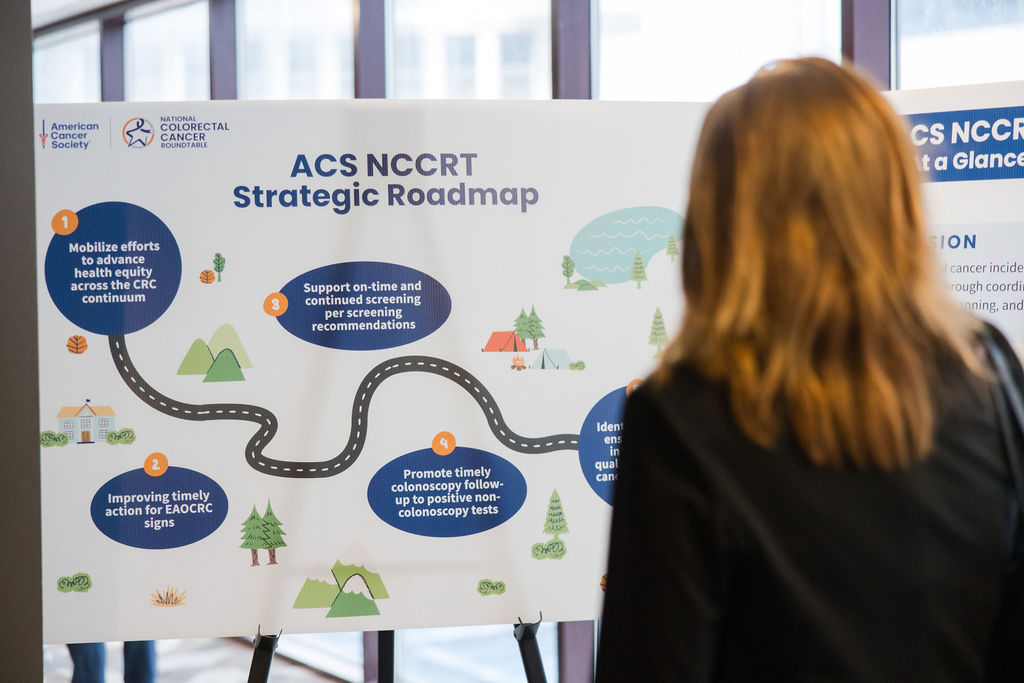
Blog: 2026-2029 Strategic Roadmap

Interview with Georgia CORE – 2025 National Achievement Award Honoree

Interview with Erie Family Health Centers – 2025 National Achievement Award Grand Prize Winner

Happy Valentine’s Day to Our Volunteers

Welcome to 2025 from Dr. Steven Itzkowitz, ACS NCCRT Chair

Interview with Unity Medical Center – 2024 80% in Every Community National Achievement Award Honoree

The ACS NCCRT Hosts Strategy Summit & Leadership Retreat to Lay the Foundation for Our Future Work
